Basic Principles of Antibiotic Use
© Michal HolubDepartment of Infectious and Tropical Diseases, 1st Faculty of Medicine, Charles University in Prague
After a careful history and clinical assessment, 10 important questions should be routinely addressed before selecting a specific antibiotic:
1. Is antibiotical treatment indicated based on clinical findings?
- Obvious bacterial infection
- Localized infections: pneumonia, pyelonefritis etc.
- Infections with characteristic clinical findings: celullitis, streptococcal tonsillitis etc.
- Inflammatory markers: leukocytosis, neutrophilia, lymphocytopenia, left shift, presence of bands, elevated C-reactive protein (CRP) and procalcitonin (PCT)
2. Urgency of the situation
- Non-urgent situation: mild infection, which does not require treatment untill the diagnosis is not established
- Urgent situation: the patient with suspected severe infection:
- Febrile neutropenia
- Bacterial meningitis
- Necrotizing celullitis
- Severe sepsis and septic shock
 |
 |
| Strawberry tongue * | Inflammed tonsils with exudate * |
 |
|
| Herpangina | |
3. Have appropriate clinical specimens been obtained, examined and cultured?
- Standard cultivation
- Gram stain
- Latex agglutination (Strep test®)
- Appropriate cultures – anaerobic and aerobic cultures
- Antibiotical treatment can be modified when the pretreatment cultures become available
- Follow up cultures are less reliable than initial pretreatment cultures
4. Which organisms are most likely to be causing the infection?
- Type of focal infection
- Age: bacterial meningitis of newborns – group B streptococci, Gram-negative bacteria
- Epidemiologic features: hospital vs. community acquired infections, prior antibiotic use, etc.
- Prior culture data: surveillance cultures in critically ill patients, immunocompromised patients, etc.
5. If multiple antibiotics are available to treat pathogen, which agent would be the best?
- Prior antibiotic allergies
- Antibiotic penetration - CNS infection, abscesses etc.
- pH - aminoglykosides are much more effective in an alkaline medium
- Potential side effects - chloramphenicol – occurrence of aplasia
- Bactericidal (bc) vs. bacteriostatic agents - in lifethreatening infections or in immunocompromised patients bc antibiotics are necessary
 |
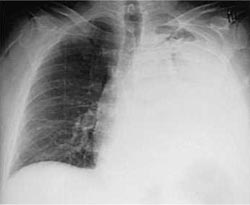 |
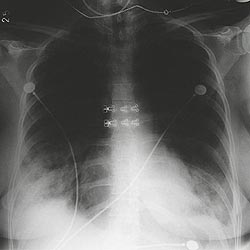
| Bacterial pneumonia | Bacterial pneumonia |
 |
 |
| Bacterial pneumonia (admission)* | Bacterial pneumonia (day 6)* |
 |
 |
| Pneumonia - Chlamydophila pneumoniae | Pneumonia - Legionella pneumophila |
 |
 |
| Pneumonia – Mycoplasma pneumoniae | Chickenpox pneumonia |
 |
|
| Erythema multiforme | |
Diagnosis of community acquired pneumonia (CAP)
- Pneumonia due to Mycoplasma and Chlamydia - procalcitonin (PCT) <0.5 ng/mL
- S. pneumoniae, L. pneumophila serotype 1 – detection of antigens in urine
- L. pneumophila - signs of disseminated infection, diarrhea and confusion
- Infection due to Mycoplasma and Chlamydia - multiform erythema, conjunctivitis, uretritis and reactive arthritis
Managing community acquired pneumonia
- Major symptoms (CURB-65)
- C - confusion
- U - urea >7 mmol/L
- R - respiratory rate >30 breaths/min.
- B - blood pressure <90 mmHg, diastolic BP <60 mmHg
- Age >65 yrs
- Minor symptoms
- Immunosuppression or severe underlying diseases (IHD, DM, CRF etc.), bilateral pneumonia, oxygen saturation <92%
- only one major symptom of CURB-65 classification = b-lactam p.o., i.m. nebo i.v. or 1st generation cephalosporin
- CURB-65 ≥2 = b-lactam + advanced macrolide
- CAP due to M. pneumoniae, C. pneumoniae or L. pneumophila = advanced macrolide (azithromycin, clarithromycin) or doxycycline (adults)
Antimicrobial-resistant bacteria:
- Penicillin resistance of S. pneumoniae
- Erythromycin resistance of S. pneumoniae
- Methicillin-resistant Staphylococcus aureus (MRSA)
- Fluoroquinolone resistance of E. coli
- Fluoroquinolone resistance of Klebsiella pneumoniae
- Carbapenem resistance of Klebsiella pneumoniae
| Penicillin resistance of S. pneumoniae | Erythromycin resistance of S. pneumoniae |
 |
 |
| Methicillin-resistant Staphylococcus aureus (MRSA) | Fluoroquinolone resistance in E. coli |
 |
 |
| Fluoroquinolone resistance in Klebsiella pneumoniae | Carbapenem resistance in Klebsiella pneumoniae |
 |
 |
European Antimicrobial Resistance Surveillance System
EARSS interactive database access
6. Is an antibiotic combination appropriate?
-
Synergism
- one antibiotc enhances the activity of another (measured by time killing curves)
- serial inhibition of microbial growth
- one antibiotic enhances the penetration of another (penicillin and aminoglycoside)
- Broad spectrum of activity – in sepsis of unclear etiology and febrile neutropenia
- Infection due to multiple organisms – intraabdominal sepsis or pelvic abscess
- Risk of drug sensitivity or toxicity
- Risk of colonization with resistant organism
- Possibility of antagonism (ie. penicillin and tetracyclin)
- High cost
- False sense of security: the use of multiple agents to cover all organisms is not possible and may be associated with complications
7. Are there special considerations related to host factors?
- Genetic factors
Pregnancy and lactation:
A. antibiotics considered safe - penicillins, cephalosporins, erytromycin base and aztreonam
B. antibiotics to be used with caution - aminoglycosides, vancomycin, clindamycin, imipenem-cilastatin and cotrimoxazole - Renal and liver functions
8. How to assess effectiveness of antibiotic therapy?
- Clinical assessment - decreased temperature - 48 hrs. for bactericidal antibiotics, 3 to 4 days for bacteriostatic drugs
- Inflammatory markers - significant decrease of CRP >25% from the baseline within 24 hrs.
- Contagiousness of patient – bactericidal antibiotics 24 hrs., bacteriostatic antibiotics - 5 days
9. Will initial therapy need modification after culture data are available?
- The antibiotic treatment should be modified if necessary based on clinical course (ie. relief of symptoms) and findings on cultivation
- Narrow spectrum of antibiotics should be used (to decrease the risk of colonization)
- Negative cultures in the patient with pneumonia and no prior antibiotics: mycoplasmal pneumonia, flu, tubercolosis, Legionnaire´s disease or opportunistic infection in immunocompromised host etc.
10. What is the appropriate dose?
| Generic name | Pediatric regimen | Adult regimen |
| Phenoxymethyl-penicillin | 50 000 IU/kg/d q4h | 800 000 UI q6h |
| Ampicillin | 25-80 mg/kg/d q6h | 500 mg q6h |
| Cephalexin | 25-50 mg/kg/d q6h | 250-500 mg q6h |
| Doxycycline | 4 mg/kg/d q12h 1 | 100 mg q12h |
| Erythromycin | 25-40 mg/kg/d q6h | 250-500 mg q6h |
| Cotrimoxazole | 30 (6) 2 mg/kg/d q12h | 960 mg q12h |
2 cotrimoxazole (trimethoprim)
References
- Reese RE, Betts RF. A Practical Approach to Infectious Diseases. 3rd edition. Boston, Little, Brown & Company 1991.
- Reese RE, Betts RF, Gumustop B. Handbook of Antibiotics. 3rd edition. Philadelphia. Lippincott Williams & Wilkins 2000.
- European Antimicrobial Resistance Surveillance System (EAARS). EAARS Annual Reports 2001 and 2007.
- Mandell GL, Bennett JE, Dolin R (eds.). Principles and Practice of Infectious Diseases, 6th edition. Philadelphia, Elsevier 2005.
- Suchopár J, Šimek R, Valentová Š et al., eds. Remedia compendium. 3.vydání. Praha, Panax Co, spol. s.r.o. 1999.
The page was last updated on September-26-2011